
In order to apply the BAIR Technique, it is necessary to familiarize yourself with the unconventional use of a common circular metal matrix. This particular use is described in the work I published in Operative Dentistry (2019; 44(4), 333-335) about a very practical and simple method for isolating class 5 lesions with cervical margins covered by gingiva.
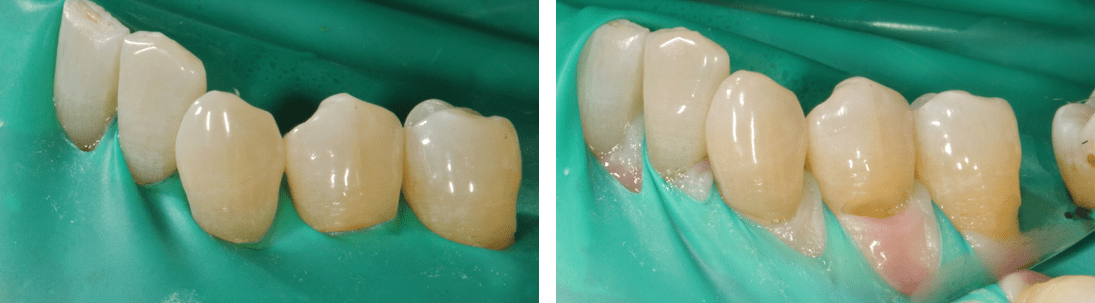
How can we proceed to isolate the lesion in cases like the one shown in the images?
Several techniques have been developed and proposed: from gingival retraction cords to the dam mounted with hooks modified and stabilized with Kerr paste, up to periodontal surgery.
The alternative (and conservative) method proposed by me not only serves to isolate the class 5 lesions, but can be used to modify the natural emergence profile of the teeth involved in the smile and for the atraumatic management of soft tissues through direct restorations. Hence it is useful not only for cervical lesions, but also for treating diastema, conoids and many other clinical situations.

This method using a circular metal matrix is able to isolate the operative site and, at the same time, move the soft tissues in the apical, mesial and distal direction, providing clear access to the intrasulcular portion of the cavity.
The procedure is very simple: after partially inserting the circular metal matrix on the tooth to be treated, passing the mesial and distal contact points, we must tilt it and push it, making it slide, towards the sulcus and keeping it adherent to the tooth. Once the edge of the matrix has engaged in the gingival sulcus, we must further push gently in the apical direction, obtaining the displacement of the soft tissues and the exposure of the cervical margin of the cavity. At this point it is possible to stabilize the matrix with wooden wedges.

Once the cavity has been isolated, we are able to easily apply the adhesive system, the flowable and the full body composite.
After finishing the restoration of the premolar, we can work in the same way on the canine.

We have a great advantage when, as in this case (shown by the arrow), the cavity extends, not only into the gingival sulcus, but also in the interproximal area, towards the mesial or distal.
Sometimes the finishing and polishing can result in some small wounds, but the consequences are extremely limited considering the subgingival extension of the cavities …